





WORLD CANCER DAY / FEBRUARY 4
Cancer is a dreaded disease, mostly detected at late stages but it can be prevented or cured, if detected early. Cancer detection has long been dependent on tumour tissue biopsies which can be obtained by surgical procedures which are both resource- and labour-intensive and are usually performed only after symptoms become clinically evident. While histopathology (microscopic study of diseased tissues and cells) remains the diagnostic gold standard, its reliance on surgical or needle-based sampling creates inherent bottlenecks for population screening, early diagnosis, and easy monitoring.
In India, a substantial proportion of cancers (~70%) are still diagnosed at advanced stages, and these limitations translate directly into delayed intervention, higher treatment costs, and poor survival outcomes. The need of the hour is to have a patient-friendly, simple diagnostic tests on easily available body fluids such as saliva, blood, and urine that enable early detection and real-time disease tracking.
NON-INVASIVE OR LIQUID BIOPSIES
Advances in molecular biomarkers-based diagnostics have moved cancer diagnosis beyond tissue-centric models towards non-invasive diagnosis using liquid biopsies. By analysing biofluids such as blood, saliva, and urine as liquid biopsies including circulating tumour DNA (ctDNA), cell-free RNA, extracellular vesicles, circulating tumour cells, microbial signatures (in virus/bacteria- induced cancers) and metabolites provide an easy and early diagnosis approach without resorting to invasive/compressive surgical procedures. These tests can be repeated over time, enabling dynamic assessment of disease evolution, therapy response, and minimal residual disease. What was once confined to only research laboratories is rapidly having wider clinical applications, driven by improvements in DNA/RNA sequencing technologies, digital PCR, bioinformatics pipelines, and now by application of artificial intelligence.
For India, the promise of liquid biopsy-based detection extends far beyond technological novelty. Non-invasive diagnostics align strongly with public health priorities by offering accessible, scalable, and potentially cost-effective tools suitable for diverse healthcare settings from tertiary cancer centres to community-based screening programmes. Their relevance is particularly very high in India as the burden of cancer is increasing, particularly for breast, cervical, oral, ovarian, colorectal, lung and pancreatic cancers, where screening coverage remains uneven and social barriers frequently delay clinical presentation. By enabling early detection and treatment, risk stratification, and monitoring through simple biofluid sampling, liquid biopsies can help shift cancer care from a reactive, late-stage model to a proactive, precision-driven early detection and effective management of cancer.
LIQUID BIOPSIES AT THE MOLECULAR CORE: DECODING TUMOURS WITHOUT TOUCHING THEM
Liquid biopsies are grounded in a fundamental biological reality: tumours continuously shed molecular materials into circulation. As cancer cells grow, die, and interact with their microenvironment, they release a spectrum of genetic, epigenetic, and metabolic signals that reflect the underlying biology and natural history of the disease. Capturing these signals allows clinicians to ‘read’ the tumour without physically accessing it.
Among the most widely studied analytes is circulating tumour DNA (ctDNA), a small fraction of cell-free DNA that carries tumour-specific mutations, copy-number changes in driver genes, and methylation patterns. With highly sensitive platforms such as digital PCR and next-generation DNA/RNA sequencing and, ctDNA can be used to detect cancer-associated alterations, estimate tumour burden, and identify emerging resistance well before clinical or radiological progression becomes apparent.
Liquid biopsies also include cell-free RNA molecules, such as microRNAs and long non-coding RNAs, which reflect dysregulated gene expression in patients. Many of these RNA species are packaged within exosomes, nanoscale vesicles actively secreted by cancer cells. Exosomes carry DNA, RNA, proteins, and lipids, and play an important role in shaping immunity and the tumour microenvironment. From a diagnostic perspective, they offer a stable and information-rich source of biomarkers, particularly valuable when ctDNA levels are very low in early-stage disease.
Another component is circulating tumour cells, rare intact cancer cells that detach from primary tumours and enter the bloodstream. Although technically challenging to isolate, they provide unique insights into metastatic potential, how stationary epithelial cells become migratory metastatic cancer cells, and therapy resistance.
An emerging frontier biomarkers analysis uses metabolites and cancer-associated microbiomes. Tumours profoundly reprogramme cellular metabolism and interact with local microbial ecosystems. Metabolomic profiles and microbial DNA signatures are increasingly linked to inflammation-driven carcinogenesis, especially in mucosal cancers such as oral, stomach, melanoma, lymphoma, etc., an area of particular relevance for India.
CHOOSING THE RIGHT BIOFLUID
The choice of biofluids requires feasibility, patient acceptability, and biological relevance. While blood remains the most widely used body fluid, saliva and urine or sputum and stool are gaining prominence due to their non-invasive nature of collection, ease of repeat sampling, and suitability for large-scale screening.
For oral and cervical cancers, these biofluids are not merely convenient but biologically meaningful and show almost 100% correlation with tissue biopsy. Saliva, in direct contact with the mouth cavity, is enriched with tumour-proximal signals. Urine offers a privacy-preserving alternative for cervical cancer screening, potentially improving participation where pelvic examinations or colposcopy-driven biopsy or smear collection pose barriers.
LIQUID BIOPSIES IN ORAL AND CERVICAL CANCERS: HIGH-IMPACT USE IN INDIA
Oral and cervical cancers together account for a substantial fraction of India’s most common cancer burden, and late-stage diagnosis remains a major challenge. Oral cancer with poor survival largely driven by delayed presentation and lacks reliable non-invasive screening tools. Current diagnostic pathways depend on visual inspection followed by tissue biopsy approaches that are impractical for early detection or community-level screening. Saliva-based liquid biopsies offer a promising solution. Tumour-derived DNA/RNA, inflammatory mediators, microbial signatures, and metabolites can all be detected in saliva, providing early molecular clues of malignant transformation. Such approaches could enable risk-stratification of oral potentially malignant disorders, helping identify individuals who need urgent biopsy versus those who can be safely monitored. Cervical cancer, despite being one of the most preventable malignancies, remains a leading cause of cancer-related deaths among Indian women. Persistent infection with high-risk human papillomaviruses (HR-HPVs) precedes invasive cancer by years, creating a window for early intervention. Yet, occurrence of more than a decade long cervical precancerous lesions also allow early detection and cancer prevention. Liquid biopsy-based detection of viral DNA, integration patterns, host methylation changes, and dysregulated microRNAs can enhance existing screening programmes. Sampling options that include urine and blood can improve compliance and allow longitudinal monitoring of disease risk.
WHY LIQUID BIOPSIES MATTER FOR CANCER DETECTION IN INDIA
High-burden cancers: Oral and cervical cancers remain major contributors to cancer incidence and mortality among both Indian men and women respectively. Liquid biopsies enable detection of tumour-derived circulating biomarkers, particularly at early disease stages, when integrated with conventional screening modalities that can achieve very high diagnostic sensitivity and specifically, enabling earlier intervention and improved clinical outcomes.
Addressing late-stage presentation: A majority of these cancers in India are often diagnosed at advanced stages, where five-year survival rates remain poor. Strategic implementation of liquid biopsy-based screening and risk-stratification models can shift detection towards early, more treatable stages, thereby substantially reducing late-stage diagnosis and improving survival outcomes.
Non-invasive and repeatable access: Saliva and urine
support safe, repeatable, and community-friendly testing, especially for patients unfit for surgery or with tumours in anatomically challenging locations. Their non-invasive nature allows frequent, real-time molecular monitoring, enabling serial assessment of tumour clonal evolution and early detection of emerging drug resistance, often months before changes appear on conventional imaging.
Smarter triage and reduced healthcare strain: Liquid biopsies act as effective triage tools, enabling rapid identification and prioritisation of high-risk individuals for confirmatory diagnostics while sparing low-risk patients from unnecessary invasive procedures.
Scalability and affordability: Liquid biopsy platforms enable high-quality cancer screening and longitudinal monitoring across diverse healthcare tiers, offering scalable, cost-effective solutions without compromising diagnostic accuracy.
BEYOND DETECTION: MONITORING AND PRECISION CARE
Perhaps the strongest clinical advantage of liquid biopsies lies in serial disease monitoring. Because biofluids can be sampled repeatedly, clinicians can track treatment response, detect minimal residual disease, and identify molecular relapse months before conventional imaging. For cancers prone to recurrence or therapy resistance, such real-time molecular surveillance can support timely, personalised clinical decisions. Importantly, liquid biopsies are best viewed not as replacements for histopathology, but as complementary tools. If used strategically, they can function as triage tests helping determine who requires immediate invasive diagnostics, who can be monitored, and who needs intensified follow-up.
SCREENING INNOVATIONS AND CLINICAL TRANSLATION: TAKING LIQUID BIOPSY FROM LAB TO LAND
The science of liquid biopsies is advancing rapidly, but their true value lies in translation turning molecular signals into actionable, scalable and affordable tools. In India, translation is shaped by three priorities: non-invasive sampling, high analytical sensitivity in early disease, and deployability across healthcare settings.
Images Courtesy: Shutterstock
Non-invasive sampling models built for scale support repeat testing and community outreach. Saliva is particularly suited to oral cancer detection, while urine-based approaches can enhance cervical cancer screening by improving privacy and participation. Because early-stage cancers shed very low levels of tumour material, modern strategies increasingly rely on multi-marker panels that integrate complementary signals ctDNA alterations, RNA signatures, exosomal cargo, metabolomic patterns, and microbial profiles to improve sensitivity while maintaining specificity. A realistic and impactful goal is to use liquid biopsies as triage tools rather than replacements for histopathology. Risk stratification can help determine who needs immediate biopsy, who can be monitored, and who requires intensified follow-up. In post-treatment settings, serial testing can track response, detect resistant clones, identify minimal residual disease, and flag early relapse. For population-level impact, platforms must match operational realities. Translation depends on affordable assay formats, standardised pre-analytical workflows (sample collection, stabilisation, transport and storage), quality control, harmonised reporting, and robust data analytics, including artificial-intelligence-assisted risk models for multi-omic signals. Without standardisation, even promising biomarkers fail to translate. With this, multi-centre adoption becomes feasible.
POLICY OUTLOOK: A NATIONAL
OPPORTUNITY TO DEMOCRATISE EARLY CANCER DETECTION
Liquid biopsies represent more than a diagnostic upgrade; they offer a strategic opportunity to reshape cancer detection in India around early diagnosis, risk stratification, and equitable access. By harnessing tumour-derived signalling molecules in blood, saliva, and urine, these platforms can shift cancer care from late-stage intervention to proactive, precision-informed early screening, early treatment and monitoring. This shift is particularly urgent for high-burden cancers such as oral, cervical, breast and lung cancers, where screening gaps and delayed presentation continue to undermine outcomes.
To convert promise into population impact, India needs a coordinated efforts and roadmap that strengthen the entire translation pipeline:
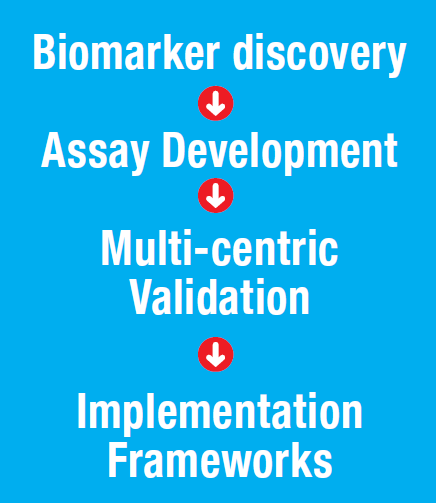
Priority must be given to large prospective cohorts, standardised sample workflows, and clinically meaningful endpoints such as early detection, progression prediction, treatment response, minimal residual disease, and recurrence risk. Equally important is implementation design: embedding liquid biopsies into well-defined clinical pathways that guide triage, referral, and follow-up, while ensuring that confirmatory diagnostics remain robust, accessible and affordable.
India is well-positioned to lead in this space because the need is urgent, the innovation ecosystem is expanding, and the benefits are clear—simpler sampling, smarter triage, earlier detection, and better follow-up. With rigorous validation, quality standards, and thoughtful implementation, the transition from invasive to non-invasive diagnostics can deliver what matters most, early diagnosis, improved survival, reduced barrier, procedural burden, and more equitable cancer care across diverse populations.
*Dr Shilpi Gupta is Assistant Professor at the Amity Institute of Molecular Medicine and Stem Cell Research (AIMMSCR), Amity University, Noida; Dr Prabhat Kumar, is ICMR-DHR-Young Scientist, AIMMSCR, Amity University, Noida; and Prof (Dr) Bhudev C Das is the Chairman, AIMMSCR, and Dean, Health Sciences, Amity University, Noida.



