





During the second wave of coronavirus infection in India earlier this year, oxygen therapy became crucial for severe patients with hypoxemia — a condition when oxygen levels in the blood are critically low. But we witnessed an acute shortage of medical oxygen in different parts of the country, from big cities to rural India. The crisis in bigger cities was more about overcoming supply chain limitations, while in smaller cities and villages, the crisis exposed a lack of medical oxygen infrastructure.
According to experts, India produces enough oxygen, at a little over 7,000 tons a day. Most of the oxygen produced is for industrial use but during the second wave, the government directed the supply of industrially produced oxygen toward the health care system. Due to high demand, suppliers ramped up capacity to be able to produce more than 9,000 tons of medical oxygen by mid-May. But the issue of transporting liquid oxygen became enormous. Most oxygen producers are based in India’s East, while the soaring demand came from every corner of the country. The transportation of liquid oxygen.
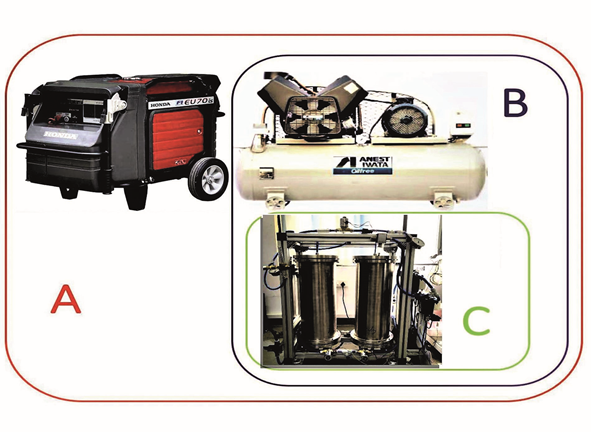
Based on the principles of the Pressure Swing Adsorption (PSA) technology, OxyJani is potentially useful in ICUs too
from the production sites to the rest of the country (in particular to cities in the North and West), by rail or road through cryogenic containers takes up to 12 days. During normal times, the mechanism of transferring oxygen from one side of the country to the other works reasonably well. However, in the face of a brutal pandemic, the market mechanism collapsed. Special cryogenic containers required to drive oxygen in large quantities across states fell short as well. These were not enough to move the entire oxygen production. There was also a shortage of cylinders, which were not being refilled fast enough to meet demands. Supplies were fixed in the very short term which resulted in an increase in price and making oxygen unaffordable and ultimately led to a high mortality rate. Though the government took measures and allowed tankers on any roads, regardless of limitations like state-specific permits, giving them priority status similar to ambulances, it wasn’t enough
Overcoming such crisis required combining the advantages of personalised oxygen concentrators for home use with a capacity of 5 to 10 litres per minute (lpm) and oxygen plants with a capacity of 500 lpm for large hospitals. The 500 lpm plants for hospitals are robust but they lack the portability required for deployment in resource-poor settings.
The personal concentrators, on the other hand, were portable but too fragile to be used on a sustained basis in hospital settings. There was a need for a robust technology with necessary portability and Indian researchers came to the rescue. A team from Jawaharlal Nehru Centre for Advanced Scientific Research (JNCASR), an autonomous institute in Bengaluru under the Department of Science & Technology, Government of India, developed a new solution with the name ‘OxyJani’ for addressing these novel challenges in adsorption science and engineering.
OxyJani is a robust, mobile group oxygen concentrator that can be used in rural settings and also be rapidly deployed in emergencies in any location. It meets the requirement, addressing, among other things, the several novel design challenges posed for the sourcing of materials. It is an entirely off-grid solution that can facilitate deployment in rural areas. The device is based on the principles of Pressure Swing Adsorption (PSA) technology.
The team replaced lithium zeolites (LiX) which is usually used in oxygen concentrators, with sodium zeolites which do not generate toxic solid waste, can be potentially a good agricultural input material.
Although the science behind Oxyjani is well understood, developing an engineering solution that can work with sodium in a portable device and fill this specific market gap when there are severe sourcing problems posed engineering challenges. Some of these included beating the obstacles at each stage of the cycle, from working with the available zeolites to effective ways of dehumidifying and designing the right adsorptionpressure cycle.
It was a multi-group initiative comprising Dr S V Diwakar, Dr Meher Prakash, and Prof Santosh Ansumali from JNCASR worked in collaboration with Prof Arvind Rajendran from the
With the robustness of large PSA plants and portability of personal concentrators, OxyJani can convert medical air to medical oxygen, and can be deployed in rural areas too
of Eiwave Digitech. The project was executed with the help of Ritwik Das, an MS student. Prof M Eswaramoorthy, Prof Tapas Maji, and Prof Sridhar Rajaraman provided technical advice. Prof G U Kulkarni, president, JNCASR, and Prof Amitabha Bandyophyay of IIT Kanpur mentored the developmental efforts. The financial assistance for the prototype was provided through JNCASR and the Nidhi Prayaas scheme of IIT Kanpur. The zeolite material used in the development of the device was obtained as a donation from Honeywell UOP, Italy.
The concentrator is modular and capable of delivering a range of solutions, conversion of medical air to medical oxygen, and is an entirely off-grid solution including all modules that can facilitate deployment in rural areas. Moreover, the waste from the 13X zeolite plant can be potentially a good agricultural input material.
This new class of technology called “group concentrators” has the robustness of large PSA plants, portability similar to the personal concentrators, and is affordable too. The device is in the range of 30-40 lpm, which is potentially useful for
ICU uses too.



