





Success of India’s COVID-19 response has a background of multiple programmes that the government of India had undertaken during 2017-18 to improve healthcare. To make India’s health sector robust, economically affordable, and accessible, the National Health Policy 2017 was rolled out. Ayushman Bharat Program (ABP), the flagship healthcare initiative, was launched in 2018 as a mission to expand universal health coverage, with a commitment to ‘leave no one behind’.
One of the components of ABP, the Pradhan Mantri Jan Arogya Yojana (PMJAY) had begun to expand the footprint of healthcare coverage to rural and vulnerable populations, improving access to hospitalisation services at secondary and tertiary level health facilities for bottom 40% of the total population. The second component of ABP was Health and Wellness Centers (HWCs), launched on 14 April 2018, and by 31 March 2020, a total 38,595 Ayushman Bharat-HWCs were operational across India. Besides, digital health initiatives had begun to evolve simultaneously. These initiatives of the government, led by Prime Minister Narendra Modi, as chairman of NITI Aayog, were significant catalyst developments in fight against the pandemic. Thus, the apex level organisational set-up existed wherein NITI Aayog was already actively engaging with the Ministries of Health and Family Welfare and AYUSH, the Department of Pharmaceuticals, the National Health Authority, state and local governments, in addition to international and national academic institutions and research organisations. Therefore, it is important to underline the fact that India’s healthcare system was prepared to take on the challenge.

Disturbing simmer of mysterious virus
Earliest indications of an inexplicable pneumonia outbreak in Wuhan seafood market had alerted the Indian intelligence and the PMO in December 2019. On 31 December 2019, WHO got to know of the cases of unknown cause and by 3 January 2020, 44 cases of hospitalization were reported in China. In parallel, PMO entrusted the responsibility to collate the information to Dr VK Paul, Member NITI Aayog, and Prof K Vijay Raghavan, Principal Scientific Advisor. As the first case of COVID-19 was reported outside China on 13 January 2020, India began thermal screening at airports for passengers coming from China on 17 January 2020.
By the first week of January 2020, the Chinese theory of animal-to-human transmission was being contested as the doubling rate of infection could not be explained and hence, the human-to-human transmission became a cause of worry. This raised an intrigue that Wuhan Institute of Virology (WIV) was not far from the market. As the COVID-19 became national news in China on 20 January 2020, WHO declared it a Public Health Emergency of International Concern. Initial apprehension that WIV had connection with outbreak gained ground as the WIV lab had been engaged in research related to SARS coronavirus since 2005 and had isolated over 300 horseshoe bat coronavirus sequences. Later, it was found that the December 2019 coronavirus cases had 96% genetic similarity to RaTG13 virus found in horseshoe bats. Although the role of WIV continues to be controversial, the early belief on the animal-man-theory of spread had proven correct for India’s science-based thinking. India reported Patient Zero on 23 January 2020 at Thrissur who had a history of train travel in China. The monster had made it to India.
India had already got its act together and by 27 January 2020, 30,000 incoming international passengers had been screened. Realising the magnitude staring at us, the government banned export of PPE kits on 31 January 2020. By late February, virus had spread had engulfed Italy, Asia and the Middle East.
First Wave Strikes
On 4 March 2020, 15 Italian tourists tested positive in Delhi and were quarantined at ITBP camp. While the modelling of COVID-19 progression was being undertaken, on the same day, the government decided to upscale Virus Research and Diagnostic Labs (VRDLs) testing facilities from 14 labs in February to 106 in March 2020. VDRL platforms provided support in handholding new laboratories for testing. Fourteen Centers of Excellence mentored approximately 300 medical colleges and finally by August, the nation had 1596 labs in India. To further meet the needs of the country, indigenous point-of-care testing was developed such as TrueNat and CBNAAT. In parallel, over 1200 NABL accredited (under ISO 1515189) private sector laboratories were rolled out. This was further augmented by point-of-care antigen testing kits which could give results in 30 minutes. And hence, the ‘test, track and treat’ became a new strategy. To take the testing material to every nook and corner of the country, ‘Mission Lifeline Udan’ transported over 40 tons of load in 150 flights during lockdown. The nation was at work!
On the other hand, on 4 March 2020, India began to brace up its might from a stockpile of only 3.35 lac N95 masks, only 2.75 lac PPE kits and only 20000 ventilators. Needless to say, India had no manufacturing capability on 4 March!
On 13 March 2020, Tablighi Jammat held a gathering of 9000 missionaries at Nizamuddin Markaz in New Delhi. Around 800 of these had participated in the congregation at Malaysia which was known as ‘super spreader event’ and Malaysia had to close its borders after this event. While the government banned a gathering of more than 50 persons in religious places, Tablighi attendees stayed put and some made way to other parts of India. Tablighi Jammat event possibly was the first ‘Super Spreader Event’ in India.
On the same day, 13 March 2020, Prime Minister called upon the SAARC nations for a collective resolve and said, “I would like to propose that the leadership of SAARC nations chalk out a strong strategy to fight Coronavirus. Together, we can set an example to the world, and contribute to a healthier planet.” Important point to note is that the call to SAARC leadership was in true spirit of Vasudhaiv Kutumbakam which India lived to its commitment when under Vaccine Maitri, doses were given to other developing countries even when we were ramping up supplies to India citizens. And, it was a foresight proven correct that COVID-19 fight is a global challenge and must be fought together. Most nations realised this approach much later, if they actually did.
India soon realised the need for strategic decision to control acceleration of case load and ‘flatten the curve’. It was most essential to make lacs of hospital beds, ICU beds, stockpile ventilators and muster healthcare workers for the surging onslaught. The idea of locking down had germinated as the indications of imminent impact were clear. Dow Jones crashed, Sensex began to crumble and events began to be cancelled. On Sunday, 22 March 2020, the partial lockdown was declared by the Prime Minister in the spirit of Jan Bhagedari. The PM introduced ’Social Distancing’, carefully nuanced in Hindi as ‘Do Gaz ki Doori’, to reflect positive connotation which became the norm later. Two days later, on 24 March 2020, at 8 pm, the Prime Minister called for a complete lockdown of the entire nation for 21 days. At that time, most nations were in a quandary and the world recognised this step taken by India as most appropriate and timely.
Vaccine Development
Globally, it is a recognised fact that the development of a vaccine can take over 15 years. India took up the task of developing COVID-19 vaccine, standardise assays, trial designs, regulatory approaches, selection of vaccine candidates, manufacture, distribution and actual vaccination at the inception of the pandemic in the country. India was quick to realise the need for development of vaccine and had confidence of its robust capacity for vaccine development. India had a successful vaccine and vaccination legacy for polio, cholera, measles, diphtheria and meningitis. India had a pioneering record of firsts in vaccine manufacture. Serum Institute of India (SII) developed first meningitis vaccine, Bharat Biotech International had launched typhoid conjugate vaccine, multi-dose inactivated polio vaccine launched by Bilthoven Biological, first fully liquid hexavalent vaccine based on whole cell pertussis developed by Panacea Biotech of India and so on. Besides, India was the only country to have over 23 pre-qualified vaccines! The ‘Atmavishwas’ had a reason to take lead.
As early as 19 March 2020, COVID-19 Research Consortium was announced jointly by the Department of Biotechnology and Biotechnology Industry Research Assistance Council (BIRAC). BIRAC eventually supported Mission COVID Suraksha and pledged Rs 900 crore for the programme. Proposals were invited for devices, diagnostics, vaccine candidates, therapeutics, and other interventions. In respect of vaccine development, three proposals were recommended for funding.
The proactive partnership in development of vaccine began to give dividends when DCGI granted first approval for Phase I and II Human Clinical Trials in July 2020, just within 4 months of the first wave. Compared to international vaccine development timelines, Moderna and Pfizer were marginally ahead of Indian candidates and published their Phase I and II trial results on 14 July and 12 August. It is pertinent to mention that Indian vaccine and vaccination programme was already in the very advanced stage before second wave struck in December 2020.
While vaccine was still about 5 months into its vaccination phase, the aggressive planning for the vaccine administration was announced on 15 August 2020. By now, the leadership of the nation was confident and began preparation for taking Suraksha Kavach to the people. It is important to note that the nation was still fighting the surging COVID-19 cases, hospital capacities and the public pressure on its healthcare delivery capacity. It is only through the convergence efforts of the union and state governments, with the partnerships with private players, that the nation was saving its people. In fact, the entire nation was unified in its resolve.
On 29 September 2020, SII declared partnership with Gates Foundation and GAVI to deliver 200 million doses by 2021. On 15 October, the Prime Minister chaired a review meeting for vaccine research and development. When India released the COVID-19 Vaccine Communication strategy on 30 December 2020, US FDA had just authorized Pfizer for emergency use on 11 December and UK gave the same approval to AstraZeneca on 30 December 2020. For India, the big day came on 3 January 2021 when emergency use approval was granted to Covishield and COVAXIN. Finally, India rolled out two of its own vaccines in Vaccination Phase on 16 January 2023. Dr VK Paul, who was at the forefront of the COVID-19 crisis from day one, took the shot on the very first day and dispelled the apprehensions of ‘vaccine hesitancy’, displayed the confidence on the achievement of the nation. India rolled out its vaccination drive in a little over 10 months. To have 4 out of the top 8 COVID-19 vaccines from India is the greatest contribution of Indian science community.
| Vaccine | Collaboration | Nation | Type of vaccine |
| Sputnik V | Gamaleya Research Institute of Epidemiology and Microbiology along with the Russian Direct Investment Fund (RDIF) | Russia | Adenovirus vector vaccine |
| PiCoVacc | Sinovac Biotech | China | Inactivated and mixed with adjuvant |
| AD5-nCoV | CanSino Biologics | China | Adenovirus-based |
| ChAdOx1-n CoV-19/Covishield | AstraZeneca/Oxford University produced by Serum Institute of India (SII) | Britain and India | Non-replicating adenovirus type 5 vector vaccine |
| BBV152/COVAXIN | Bharat Biotech in collaboration with ICMR and NIV (Pune) | Hyderabad, India | Inactivated whole virion candidate vaccine |
| ZyCoV-D | Zydus Cadila | India | DNA plasmid vaccine |
| NVX-CoV2373 | Novavax vaccine manufactured by SII, India with annual production of a billion doses | USA and India | Glycoprotein sub-unit (recombinant protein) nanoparticle adjuvanted vaccine (matrix M) |
| BNT162 | Pfizer/BioNTech | USA | Three lipid nanoprotein mRNAs |
The Nobel Prize 2023 in Physiology or Medicine has been awarded to Katalin Karikó and Drew Weissman for their discoveries concerning nucleoside base modifications that enabled the development of effective mRNA vaccines against COVID-19. However, Indian scientific, medicine, vaccine collaborations, vaccination programme leadership and participants in delivery system deserve greater recognition.
The Vaccination Drive
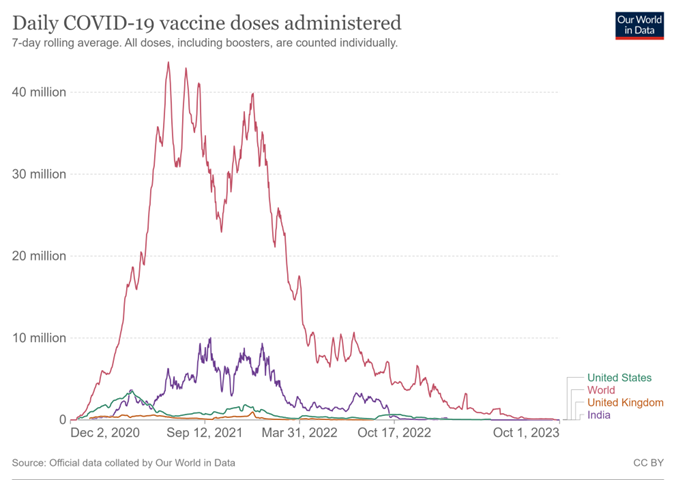
Vaccination in India was certainly not an easy task. The meticulous preparation to reach geographically diverse locations, inaccessible, challenging terrains had started as early as 15 August 2020 while the actual vaccination drive stated on 16 January 2021. Vaccination drive of India was the biggest, unparalleled and historic in the world and over 220 crore doses were administered, the fastest ever. Indian vaccination program saved 34,22,00054 lives due to its vaccination programme as reported in an independent Lancet research on modelling by Stanford University and the Institute of Competitiveness. User interface, vaccination certificate and entire monitoring became possible in real time without digital support. To ensure that no one was left out, CoWIN digital platform was conceived as the robust backbone for India and offered to other countries as well. Vaccine administration has been nearly equal by gender. Covishield was administered the most, followed by Covaxin and Corbevax in very limited doses.
Source: https://ourworldindata.org/covid-vaccinations
India started to export vaccines as Vaccine Maitri initiative and delivered 16.29 crore doses to 96 different countries as humanitarian assistance. The cost of Indian vaccination was under 3 USD, lowest as compared to other developed nations with efficacy of Covishield as nearly 90%, Covaxin as 78% and Corbevax >90%. Adverse Events Following Immunisation (AEFI), the complications reported after receiving the vaccine in India, was around 0.006 per cent while in the US it was 0.2% and in UK it was 0.7% as per affidavit filed by the government in the Supreme Court of India.
Vaccine development and vaccination was the perfect example of Atmanirbharta, executed with Atmavishwas and in the spirit of Vasudhaiv Kutumbakam.* This article is based on the excerpts of the lecture, ‘COVID-19 Vaccine Journey: Lessons in Science and Delivery’, delivered by Dr VK Paul, Member, NITI Aayog, at INSA, New Delhi.



